The 2018 Pumphandle Lecture will be held at 17.30 on Thursday 6th September 2018 at the London School of Hygiene and Tropical Medicine.
The Society is proud to annouce that Dr Joanne Liu, International President of Médecins Sans Frontières (MSF)/Doctors Without Borders, will be speaking at the 2018 Pumphandle Lecture on ‘The Cost of Fear: humanitarian crises in the age of anxiety’.
The lecture is free, but tickets are required and are now available. We encourage early booking to ensure a space.
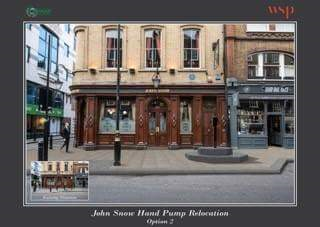
Many members will know that the replica pump which was placed by Westminster Council at the corner of Poland and Broadwick Streets in 1992, to commemorate our hero’s work, was removed in 2015 because of construction. The Society has worked tirelessly over the past three years to ensure its return – and to the historically proper position. We can now report success, as the pump, appropriately without handle, was unveiled at its new and correct site on Friday 20th July 2018. A small ceremony took place at 0800 on that day, at which time Dr Ros Stanwell Smith, our Society’s Pumphandle Ambassador, gave a short speech and Councillor Richard Beddoe removed a sheet uncovering the pump. The event led to a storm of approval on social media.
The plaque reads as follows:
“Dr John Snow (1813 – 1858) a noted anaesthetist and physician, lived near the focus of the 1854 Soho cholera epidemic, which started in August 1954 in Broad Street, as Broadwick Street was then called. In September of that year more than 500 people died in Soho from the disease.
Snow had studied cholera in the 1848-9 epidemic in South London and developed a novel theory that polluted drinking water caused the disease. He recognised that cholera cases were clustered around the water pump located here and showed it was the cause of the epidemic.
His theory initially met with some disbelief but he convinced the parish council to remove the pump’s handle on 8th September 1854, to prevent its further use. ‘Removal of the pumphandle’ has become an international symbol of public health. The John Snow Society was founded in 1992 to commemorate Snow’s work.
The original pump was situated outside the site where the ‘John Snow’ Public House now stands, and this replica has been returned to its historic location previously marked by a pink granite kerbstone.
This water pump was unveiled by Cllr Richard Beddoe On 20 July 2018 It marks a pioneering example of medical research in the service of City of Westminster”
Members with a particular concern for detail will be pleased to note that the pink granite kerbstone has been incorporated into the installation, immediately west of the pump’s plinth.
A replica of the infamous John Snow pump has been reinstalled on Broadwick Street in Soho, and will be unveiled at the Broadwick Street (John Snow) Pump Unveiling, this Friday, 20th July at 8am.
Rosalind Stanwell-Smith, Trustee of the John Snow Society, and Cllr Beddoe, Westminster City Council Cabinet Member for Place Shaping and Planning, will speak briefly before unveiling the newly refurbished pump.
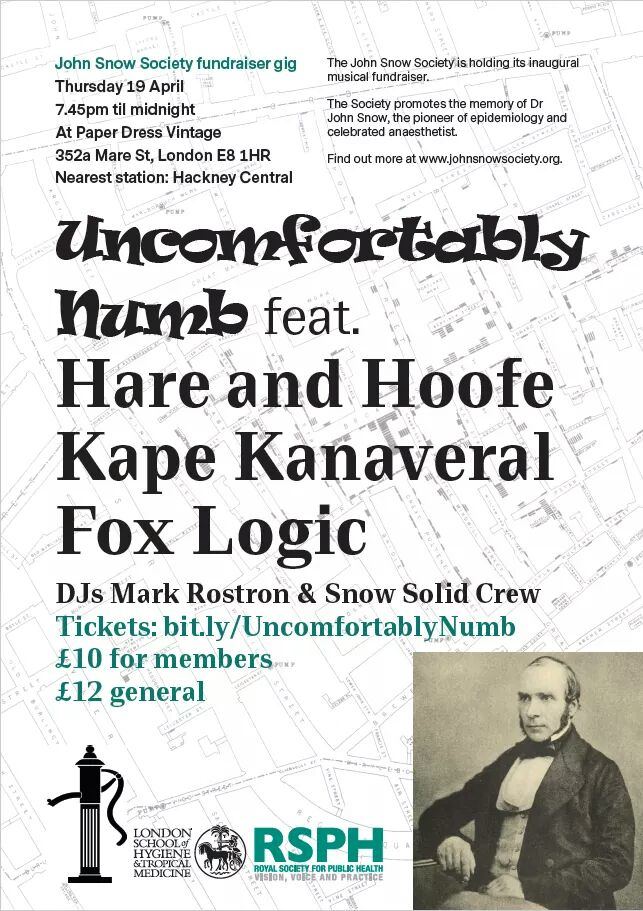
April 19th 2018 from 7.45pm at Paper Dress Vintage, 352a Mare St, London E8 1HR
The John Snow Society is holding its inaugural musical fundraiser, featuring performances by The Hare and Hoofe, Kape Kanaveral, LIND, and Fox Logic, and DJs Mark Rostron and Katie Steels! The event will be held on 19th April 2018, from 7:45pm – midnight at Paper Dress Vintage, 352a Mare St, London E8 1HR http://paperdressvintage.co.uk/.
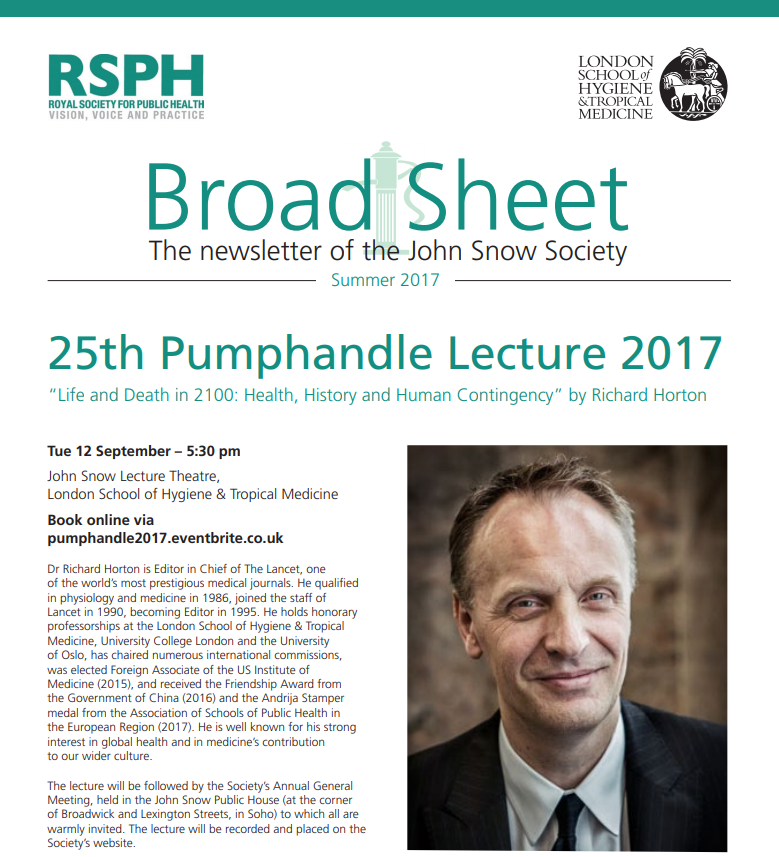
The 25th Annual Pumphandle Lecture was delivered on 12th September 2017, by Dr Richard Horton, Editor in Chief of The Lancet.
This was a broad and passionate critique of global heath and today’s world. Dr Horton began by emphasising a fundamental principle of evolutionary biology which guides selection for altruistic behaviour: “rB>C” where r is relatedness, B is benefit and C is cost. In effect the more distantly related are two individuals, then the greater the benefit must be of an action if it is to be worth doing (ie to exceed its cost). He then reviewed the contrast between techno-utopian (ever increasing healthy life expectancy, robots for everything…) versus the dystopic (2 billion climate refugees by 2100, unsustainable environments, heightened extinction risks…) visons of our future, and related this to historical trends, in particular the evolution from the optimism of the 17th century enlightenment, to the desperate circumstances of urban environments in the early industrial revolution and political reaction, to the consequent anger and despair of the romantic movement. References to Aimee Cesaire, Francis Bacon, John Rawls and Amartya Sen were cited to illustrate these tensions and point to the importance of dialogue and communication between peoples.
At this point our speaker referred to his own experience as editor of a major journal, which publishes much in the area of global health, and regretted that so much of the reality of the contemporary communication industry was concerned with survival and impact factors and profit and competition, with too little concern for purpose and meaning of the larger enterprise. Too much concern for human rights which focuses upon our rights over others… too much focus upon the extremism of others but not of ourselves… too much concern over the “post truth” world without sufficient concern for the brutal facts of the lives of others.
Turning to solutions he referred to the usual calls for equity and the right to health … but stressed the overall importance of solidarity, or the degree of social cohesion – hence returning to his original reference to rB>C, stressing the importance of relatedness and the need to expand this beyond simple genetics to all humanity. We in the health professions have much to contribute, as health is one of the greatest levers for creating solidarity between all peoples. This is turn will require moving beyond simple objective descriptions of our subjects and study participants, as in so much contemporary research, to sympathetic appreciation of the plight of others and of our common humanity. To help meet this challenge he announced that The Lancet would start a new series exploring personal experiences.
He concluded by referring to the great romantic William Blake, who was born very near to the Broad Street pump, and who noted that “what is now proved was once imagined”.
The vote of thanks was proposed by Professor Jimmy Whitworth, and Dr Horton was invited to remove the handle of the pump to close the proceedings. Society Members then adjourned to the John Snow Pub in Soho for the Annual General Meeting of the Society.
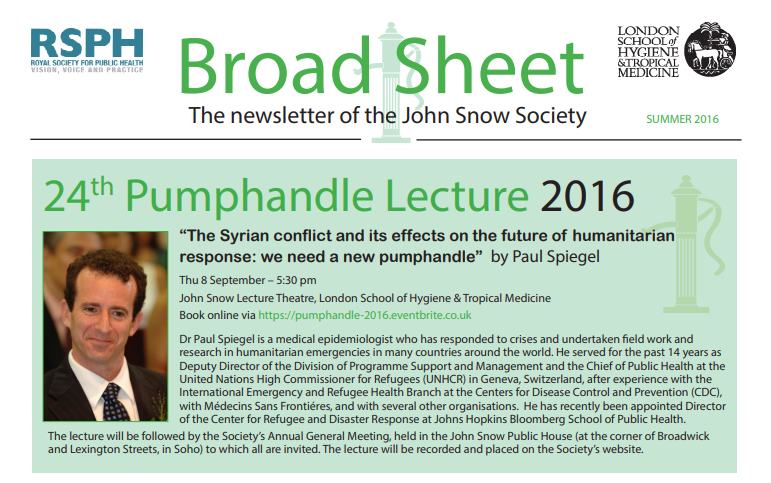
Paul Spiegel on the need for a new pumphandle in humanitarian crisesThe society is proud to have hosted Paul Spiegel with his lecture on “The Syrian conflict and its effects on the future of humanitarian response: we need a new pumphandle”. A record number of ticket reservations for this event was recorded. As usual, the lecture was followed by the AGM in the John Snow pub, this time with a truly memorable 54(-ish) words interactive song on John Snow, stated for the successful application for membership of the J3SC.
The 24th Annual Pumphandle Lecture was delivered on 8th September 2016, by Dr Paul Spiegel, recently appointed Director of the Center for Refugee and Disaster Response at Johns Hopkins Bloomberg School of Public Health. Previous to this appointment, Dr Spiegel had spent 14 years as Deputy Director of the Division of Programme Support and Management and Chief of Public Health at the United Nations High Commissioner for Refugees (UNHCR) in Geneva.
Dr Spiegel began by referring to the large numbers of refugees and displaced persons in the world today – the largest numbers since the Second World War, with the majority coming from Syria, Afghanistan and Somalia. He commented on the history of such humanitarian crises in recent decades, from Biafra in the 1960s to Cambodia in the 1970s to the many states in crisis today. Circumstances have changed considerably over the years both in the nature of the crises and countries where they take place, and the various institutional responses. Much of the data come from refugee camps, and it has been difficult to quantify populations affected but not in camps. Crises have become protracted and health problems have shifted from a focus on communicable disease to a wide variety of health problems including those associated with middle income populations such as in Syria. New agencies have arisen, several within the UN but many with other international, national or local bases. Recently several Islamic agencies have become involved, and there is a move for private sector involvement. Coordination of all these agencies has posed problems and it is recognised that decision-making has not always been optimal, having to be made on imperfect data in a complicated political context.
He devoted much of the lecture to expanding details on five recommendations he considered essential for the improvement of responses to such crises. First is the need to “Operationalise the concept of centrality of protection”, recognising the priority to provide a safe environment for people but appreciating the complexity of this challenge. Second is the need to “Integrate affected persons into national health systems” making use of the talent and experience of the displaced persons. Third is a need to “Remake, not simply revise leadership and coordination”. He argued that the WHO has justifiably held a central position on the global stage but that it has failed repeatedly in recent years – it must repair its structures and procedures soon, or lose its central position. Fourth is the need to “Make interventions more efficient, effective and sustainable” which has many implications, including the need to move from annual budgets and short term thinking to recognition of need for long term infrastructure and the importance of education and livelihoods for societies if they are to survive and prosper.
Finally he referred to the need for “Data and research to improve outcomes and impact”. The need for effective evidence-based decision-making is obvious – but this requires systematic collection and critical analysis of data in order that the required evidence can accumulate. He referred in particular to the Wellcome Trust / DfID R2HC initiative (on “Research for Health in Humanitarian Crises”) which is encouraging rigorous research on this group of problems. Dr Spiegel closed by referring to what he called the “forgotten emergencies” in countries such as South Sudan and Central African Republic, which have been crowded off the global agenda because of the magnitude and urgency of the crises in and around Syria. The world has failed both in allowing these circumstances to arise, and in responding to them. Something new is required to deal with these immense problems– a new pumphandle.
The vote of thanks was proposed by Professor Jimmy Whitworth, and Dr Spiegel was invited to remove the handle of the pump to close the proceedings. Society Members then adjourned to the John Snow Pub in Soho for the Annual General Meeting of the Society.
‘The Society of Anaesthetists: a Methodological Approach to its History’ – John Snow Society members invited to join lecture for free.
Members of the John Snow Society are invited to join the lecture from the History of Anaesthesia Society on ‘The Society of Anaesthetists: a Methodological Approach to its History’ for free. This Blessed Chloroform Lecture will be delivered at their annual meeting to be held just outside Oxford at the Hawkswell House Hotel on Saturday 2nd July at 11.30 am.
The Blessed Chloroform Lecture does not require booking – the History of Anaesthesia Society’s other lectures during their Oxford Meeting will be charged at the normal rate and require booking and payment: http://www.histansoc.org.uk/events.html